

Photobiomodulation Therapy
Does the term “laser” therapy make you think of Dr. Evil using his quotation marks and threatening to blow up world with a giant “laser” and wondering how this is possibly going to help your pain? If so, that was me also initially.
I was put on to laser therapy by a fellow interventional and regenerative pain practitioner colleague who had started using it in his own clinic and was noticing some very impressive results. After discussing it with him I decided to look into things further.
Laser therapy has gone by many names over the years including; cold laser, low level laser therapy (LLLT), low-power laser therapy (LPLT), biostimulation just to name a few. These days the agreed upon term is Photobiomodulation Therapy (PBMT) as this more accurately encompasses the use of light waves/photons to stimulate biological changes for therapeutic reasons, without references to power levels and the like.
When I started looking into PBMT, I was surprised to find that just like a lot of the other treatment techniques that I use, there was actually a surprising amount of scientific data regarding the use of PBMT therapy to treat various medical conditions, with most in the setting of healing.
The first published scientific data on Laser therapy goes all the back to 1967 when Andre Mester irradiated mice with a low energy Ruby laser (694 nm) to see if it might cause cancer. To monitor the response, he shaved the hair off the backs of the mice. He was surprised to find that there was no increase in cancer but the only significant change was that the hair on the treated mice backs grew back faster! He called this “Laser Biostimulation” (Mester et al, 1967).
Since 1967 over 100 phase III, randomized, double-blind, placebo-controlled, clinical trials (RCTs) have been published and supported by over 1,000 laboratory studies investigating the primary mechanisms and the cascade of secondary effects that contribute to a range of local tissue and systemic effects (Huang et at, 2009).
The treatment is completely painless and side effects are extremely rare. Reports from multiple other clinicians that I spoke with prior to deciding to proceed with PBMT treatments reported that about 80-95% of patients got significant benefit with laser therapy. Most of these seem to have a very noticeable benefit (~65-70%) with about 20-25% having a mild improvement.
It can take 3-6 treatments for the benefit to become clear. Even better results can be achieved when the laser therapy is combined with other treatment techniques. At Nexus Pain Management, each patient will be presented with options for their particular case and they can decide what is right for them after understanding the pros and cons of each approach.
What is photobiomodulation or Low Level Laser Therapy (LLLT)?
Low level laser therapy (LLLT) is defined as the application of light (usually a low power laser or LED in the range of 1mW – 500mW) to a pathology to promote tissue regeneration, reduce inflammation and relieve pain. The light is typically of narrow spectral width in the red or near infrared (NIR) spectrum (600nm – 1200nm), with a power density (irradiance) between 1mw-5W/cm (Agaiby et al, 2000). The treatment is applied for a minute or 2 at each location about 2-3 times per week for a few weeks.
Randomised control trials into LLLT have shown benefits with
Osteoarthritis
Tendinopathies
Back pain
Neck pain
Muscle fatigue
Nerve injuries and neuropathic pain
Wound healing
Just to name a few.
There is also some interesting emerging data in spaces like traumatic brain injury, Stroke, Alzheimer’s and many other conditions that may also be helped by PBMT.
One small note is that not all studies (especially in the early days) have shown benefit. Over time as scientists learnt more and more about the effects of PBMT on human tissue. This has now allowed protocols to become more refined and with this the literature seems to show a consistent benefit when the therapy is applied as per standard protocols, but it is an ever evolving field.
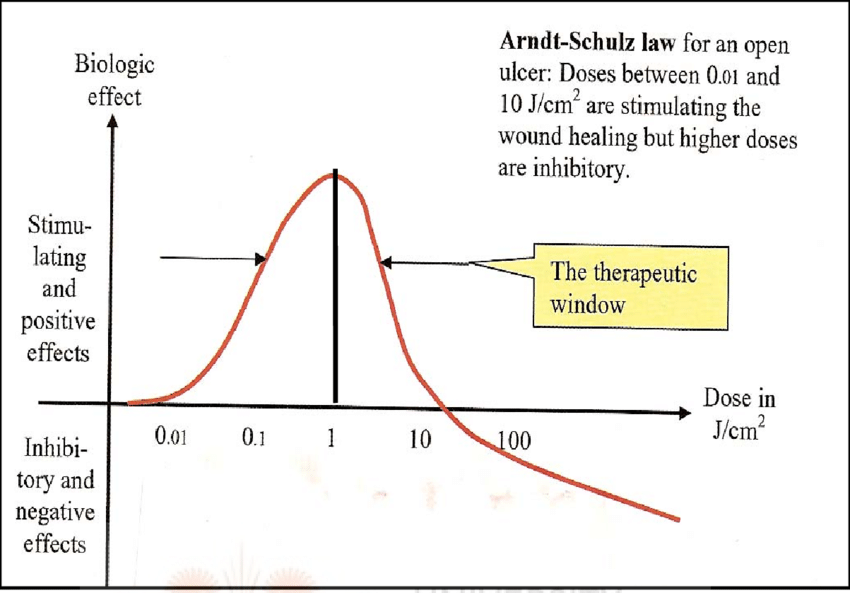
One important element regarding the success of laser therapy relates to dosing. Laser therapies will have a biphasic (or Arndt-Schulz) curve of effect with regards to benefit and harm with laser treatment.
Tuner, J. and Hode, L. (2002) Laser Therapy—Clinical Practice and Scientific Background. Prima Books, Grangesberg.
This means it is not a simple case of more is better. Basically, not enough irradiation won’t help much, but too much can also be unhelpful and potentially even mildly damaging, so simple blasting away is also not a good idea. There is a “sweet spot” of treatment irradiance that is best for optimal healing and this is generally in the dose range of 0.1-10J/cm2 range. I will cover that in more detail below.
How does it work?
The quick summary is that NIR light will result in increased energy levels for cells and increased production of growth factors and enzymes that assist in healing. The detailed explanation of the mechanism is below.
The human chromophore (a molecule which absorbs light at a particular wavelength and reflects colour as a result) of the human body will dictate how much NIR light will reach the underlying tissues and their biological effect. You can see the spectrum of the human chromophore below as well as the levels of absorption/reflections of biological components (melanin, haemoglobin, water). You will note that most laser systems use some common wavelengths for this reason where there is a natural dip in the absorption/reflection of melanin, haemoglobin or water to optimise penetration and treatment depth.

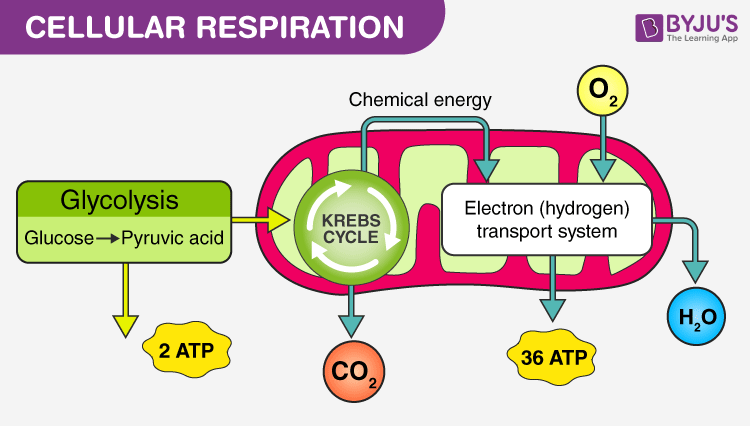
The healing effects of irradiation of tissue with light in the 600-1200nm range is mostly related to the effect of the light on an enzyme in the mitochondria (which creates energy for our cells) called cytochrome c oxidase (CCO). It is the 4th enzyme in the electron transport chain that each cell in our body uses to turn energy sources, such as glucose, into adenosine triphosphate (ATP). ATP is the energy source that our cells actually use.

Complex IV = Cytochrome c oxidase
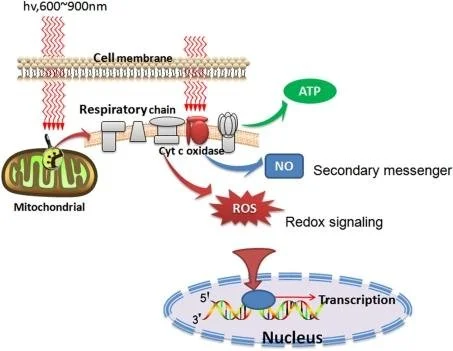
The result of NIR light being absorbed by cytochrome c oxidase (CCO) is that it facilitates the dissociation nitrous oxide (NO) from CCO and this will in turn
1) alter mitochondrial membrane potential and increase ATP (cellular energy) synthesis
2) increased free nitrous oxide (NO) levels
3) alter levels of reactive oxygen species (ROS)
4) Increase transcription and production of growth factors and enzymes (as enzymes react to changes in cell redux. Cell redux is that balance of reactive oxygen and nitrogen species)
Huang et al 2011
In the 800-820 nm wavelength range there is a natural dip in the absorption of melanin, haemoglobin, water with good absorption for CCO. Therefore, this is a very important wavelength for the energy related effects from cytochrome c oxidase but minimal absorption, meaning better penetration into the tissues. Other wavelengths will have some effect on CCO but will also have other effects. 905 nm light can help dissociate oxygen from haemoglobin helping to oxygenate tissues. 970 nm light can have some effect on CCO as well as calcium channels and its absorption by water can aid with gentle warming which can allow blood vessels to open and improve blood flow as well as improve venous return to reduce swelling. 1064 nm light is especially important for those with darker skin tones (lots of melanin) as the lower wavelengths are more heavily absorbed. 660nm light has benefitcial effects but is limited by reduced benetration nto the skin (~0.5-1cm). However, it if good for healing in these superficial tissues including scar tissue and wounds.
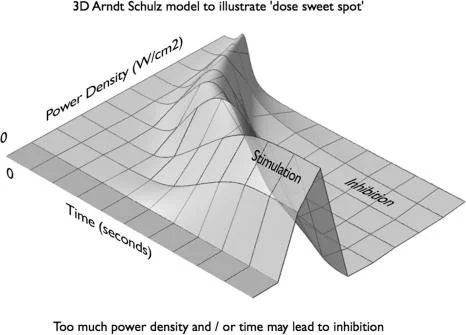
As mentioned previously, dosing is also an important factor if the effectiveness of LLLT. An example of stimulation versus inhibition of healing at varying doses of laser therapy is shown below. Which makes sense in that if you are dissociating NO from CCO and altering the balance of free NO, reactive oxygen species and ATP formation (which affects the membrane protein gradient) when doing this excessively will likely push the cell too far and the subsequent changes could even damage or destroy the cell.
Huang et al 2011
Due to the potential complexity regarding LLLT dosing, we at Nexus Pain Management have taken extra precautions to make sure we get things right. Firstly, all clinical staff that operate the laser much have undergone additional training in laser therapy to ensure safety and effectiveness. Dan has done an extensive research into the PBMT space investigating multiple machines and seeking independent advice on the best units for his patients.
After much careful thought we decided to use the K-laser speciale rather than other units for a few important reasons.
1. Wavelengths
6 wavelengths as opposed to most units 1 or 2. As mentioned above each wavelength can have its own benefits and having 6 options allows for better adaptability for a given patient
2. Power
40W average power vs most others in the 5-10W range with well-defined protocols to ensure dosing in the correct range. So as the graph above shows this allows a much shorted treatment time as adequate energy levels are absorbed faster.
3. Advanced dose monitoring sensors
The K-laser speciale is the first model in the country to have advanced dose monitoring and AI guidance to specifically monitor patients skin colour and temperature and automatically adjust machine parameters to ensure the patient is getting the optimal treatment
4. Customisable options
K-laser is also the only system that has completely customisable options. This means that if a study comes out in future with a profound benefit, the K-laser system can then reproduce the exact settings as per the study rather than being locked in to existing settings as are other units
5. Extended training
K-laser has a research institute in Italy that is constantly studying and modifying protocols. There is also extended training provided to ensure practitioners are able to get the best out of the machine for patients
The K-laser product is well regarded in the laser therapy space and is the recommended unit of the The Laser Therapy Institute in the USA, which is an independent clinical body that provides extra training in laser therapy treatment.
-
Mester E, Szende B, Tota J.G. Effect of laser on hair growth of mice. Kiserl Orvostud. 1967;19:628–631.
Agaiby AD, Ghali LR, Wilson R, Dyson M. Laser modulation of angiogenic factor production by T-lymphocytes. Lasers Surg Med. 2000;26(4):357-63. doi: 10.1002/(sici)1096-9101(2000)26:4<357::aid-lsm3>3.0.co;2-o. PMID: 10805940.
Huang YY, Sharma SK, Carroll J, Hamblin MR. Biphasic dose response in low level light therapy - an update. Dose Response. 2011;9(4):602-18. doi: 10.2203/dose-response.11-009.Hamblin. Epub 2011 Sep 2. PMID: 22461763; PMCID: PMC3315174.
Sommer AP, Pinheiro AL, Mester AR, Franke RP, Whelan HT. Biostimulatory windows in low-intensity laser activation: lasers, scanners, and NASA's light-emitting diode array system. J Clin Laser Med Surg. 2001 Feb;19(1):29-33. doi: 10.1089/104454701750066910. PMID: 11547815.
Tuner, J. and Hode, L. (2002) Laser Therapy—Clinical Practice and Scientific Background. Prima Books, Grangesberg.
For those interested in extra scientific reading into PBMT. Here are some of the pertinent articles that I have found over time.
For those who would like to deep dive into LLLT treatments and how they work, as well as the dosing considerations there are 2 excellent review articles by Huang et al in 2009 and 2011 and I would strongly encourage reading them as a starting point
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2790317/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3315174/
This article also is a good summary on PBMT and goes into more detail especially with MSK conditions and Fibromyalgia- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9980499/
This article is another good summary of the mechanism of action and dosing - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4743666/
Some more detailed mechanism of laser and dosing in mice - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6037550/
This blinded study uses PBMT to the stellate ganglion to treat PTSD - https://www.jstage.jst.go.jp/article/islsm/9/1/9_1_7/_pdf#:~:text=Results%20demonstrate%20that%20laser%20irradiation,true%20effects%20of%20laser%20irradiation.
Trigeminal neuralgia - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4091693/, https://dentjods.sums.ac.ir/article_49081_ba7398d367071e69324a20b4b4cb431d.pdf
neck pain - review – Lancet - https://pubmed.ncbi.nlm.nih.gov/19913903/
knee arthritis - review – BMJ - https://bmjopen.bmj.com/content/9/10/e031142
nerve repair - https://link.springer.com/article/10.1007/s10103-004-0300-3, https://pubmed.ncbi.nlm.nih.gov/17603852/
Analgesia via neural blockade - https://pubmed.ncbi.nlm.nih.gov/17374099/#:~:text=830%20nm%20laser-,830%20nm%20laser%20irradiation%20induces%20varicosity%20formation%2C%20reduces%20mitochondrial%20membrane,effects%20of%20830%20nm%20laser
Summarises PBMT wavelengths and effects on wound healing including increasing growth factors - https://pubmed.ncbi.nlm.nih.gov/23636299/